
[ad_1]
The recognized: People with suspected coronary artery illness (CAD) in rural or distant Australia are sometimes referred to metropolitan hospitals for invasive coronary angiography (ICA), incurring substantial prices and inconvenience.
The new: Of 1017 individuals from rural or distant Western Australia referred for ICA in Perth, one‐third had non‐obstructive CAD and two‐thirds didn’t require revascularisation. Computed tomography coronary angiography (CTCA) in rural centres might determine non‐obstructive CAD and consequently avert 53% of referrals and scale back well being care prices by $7.3 million (36%).
The implications: Providing CTCA in rural centres might enhance entry to cardiac providers and scale back the prices related to sending individuals for ICA in Perth.
Coronary artery illness (CAD) is a number one reason for morbidity and mortality.1 The burden is bigger and affected person outcomes are poorer in rural and distant Australia than in metropolitan areas.2 One essential issue is the restricted entry to specialist cardiac care in much less populated areas. Western Australia is characterised by giant distances between its rural centres and metropolitan hospitals. People with suspected CAD in rural or distant areas are sometimes transferred by air to metropolitan hospitals for cardiac investigations reminiscent of invasive coronary angiography (ICA), an strategy related to substantial prices, process‐associated issues, and inconvenience for the affected person.3,4 As many individuals who bear ICA shouldn’t have obstructive CAD or want revascularisation, different, non‐invasive danger stratification methods are wanted.5
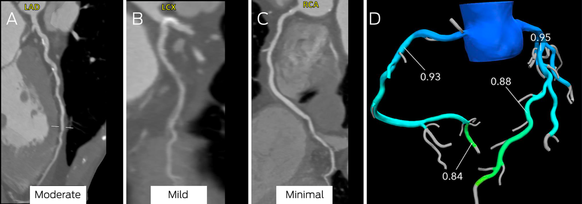
Computed tomography coronary angiography (CTCA) is a non‐invasive imaging modality for comprehensively evaluating the burden and severity of CAD.6 CTCA can detect excessive danger plaque and assess lesion‐particular ischaemia utilizing the usual acquisition and computed tomography (CT)‐derived fractional circulate reserve (CT‐FFR) respectively.6,7 Making CTCA obtainable in rural centres with 64‐slice (or higher) CT scanners (, determine 1) would enhance entry to cardiac providers.8 CTCA might additionally determine individuals with non‐obstructive CAD who don’t require switch to metropolitan hospitals for ICA. However, the prices of creating CTCA amenities in rural Australia haven’t been evaluated.6
We investigated the severity of CAD in individuals from rural or distant Western Australia referred for ICA in Perth and their subsequent administration. We additionally estimated the potential value financial savings have been CTCA obtainable in rural centres for first line investigation of individuals with suspected CAD.
Methods
We undertook a retrospective cross‐sectional examine of adults (18 years or older) referred from rural and distant WA hospitals and first care centres to the three public tertiary hospitals in Perth (Fiona Stanley, Royal Perth, Sir Charles Gairdner Hospitals) for ICA analysis of suspected CAD throughout the 2019 calendar yr. This was the latest yr wherein hospital useful resource ranges and medical choice making weren’t influenced by the coronavirus illness 2019 (COVID‐19) pandemic. “Rural” and “remote” have been outlined in keeping with the Modified Monash Model.9 We extracted affected person knowledge from digital medical information, together with discharge summaries and the central angiography database for all public hospitals in WA. We excluded individuals with unstable displays (ST‐elevation myocardial infarction, cardiac arrest, cardiogenic shock, unstable arrhythmia), in addition to individuals who have been referred for elective revascularisation, had been evaluated for CAD throughout the previous three months, or for whom knowledge have been incomplete. We labeled indications for ICA as non‐ST elevation myocardial infarction (NSTEMI), chest ache with regular troponin ranges, or different (evaluation of valvular coronary heart illness, arrhythmia, or cardiomyopathy).
Coronary artery illness: traits and administration
Severity of CAD was derived from data in ICA experiences. Stenosis severity was outlined in keeping with the coronary artery illness reporting and knowledge system (CAD‐RADS), based mostly on essentially the most extreme stenosis detected: no stenosis (0%), minimal (1–24%), delicate (25–49%), average (50–69%), extreme (70–99%, or > 50% in left principal coronary artery), and occluded (100%).10 Management was categorised as medical or revascularisation (percutaneous coronary intervention or coronary artery bypass graft surgical procedure). The effectivity of ICA useful resource use was outlined by the ICA:revascularisation ratio.11 We assumed 99% sensitivity and 88% specificity for CTCA detecting obstructive CAD (≥ 50% stenosis), based mostly upon a subset of sufferers in a meta‐evaluation wherein ICA was the reference evaluation technique.12
Health care prices
The three well being care system value elements for the yr 2019 we assessed (, desk 1) have been:
- the price of switch from a rural or distant location to a metropolitan hospital;
- the price of the metropolitan hospital admission, based mostly on size of keep; and
- the price of ICA with or with out revascularisation.
For inter‐hospital transfers, Royal Flying Doctor Service prices have been obtained from the WA Country Health Service. For elective transfers, the fee was calculated as the utmost affected person subsidy offered by the WA Country Health Service for self‐funded journey in keeping with location and distance. Costs of the hospital admission, ICA, and revascularisation have been estimated utilizing prognosis‐associated teams (DRG) codes obtained from the WA Health Business Team.
Based on the Medicare Benefits Schedule (2019), the price of CTCA was estimated to be $716.90 (merchandise 57360) and of stress echocardiography $656.85 (gadgets 55132, 55143). The time of misplaced productiveness was deemed to be equal to the size of the metropolitan hospital keep, and revenue misplaced for individuals of working age (15–64 years) was calculated from Australian Bureau of Statistics age‐ and intercourse‐adjusted incomes knowledge for 2018–19 (, desk 2).13
Alternative care mannequin: native computed tomography coronary angiography
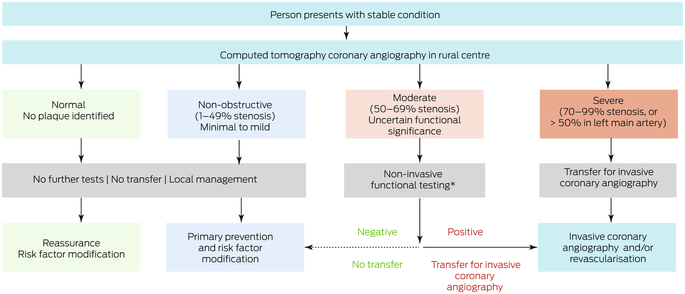
We additionally examined a possible different mannequin of take care of which we assumed that CTCA could possibly be carried out in rural centres (Box 1). People with regular or non‐obstructive CAD (< 50% stenosis) in keeping with CTCA wouldn’t require ICA and consequently not be transferred to metropolitan hospitals, however these with extreme CAD (≥ 70% stenosis) could be transferred. People with average CAD (50–69% stenosis) would bear purposeful testing (stress echocardiography or CT‐FFR) within the rural centre; for the purposeful testing final result we used the precise revascularisation final result. We in contrast well being care prices for typical care (ie, as decided by retrospective assessment of medical information) and for the choice care mannequin (simulated rural CTCA outcomes based mostly on people’ precise ICA findings).
Statistical evaluation
Analyses have been carried out in SAS 9.4. We summarise knowledge as means with customary deviations (SDs), numbers and proportions, or medians with interquartile ranges (IQRs). Associations of CAD severity and remedy with indication for ICA have been assessed utilizing binary logistic regression evaluation and reported as odds ratio (ORs) with 95% confidence interval (CIs). P < 0.05 was deemed statistically vital.
Ethics approval
This examine was accredited as a medical audit by the South Metropolitan Health Service (Western Australia) Governance, Evidence, Knowledge and Outcomes committee (FSFHG GEKO42539).
Results
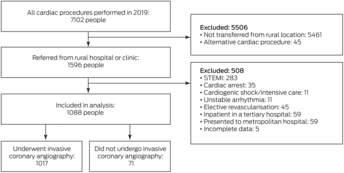
Of 1596 individuals from rural or distant WA referred for ICA in Perth throughout 2019, 508 have been ineligible for our examine and 71 didn’t bear ICA (Box 2). The imply age of the 1017 individuals who underwent ICA was 62 years (SD, 13 years), 680 have been males (66.9%), and 245 have been Indigenous individuals (24.1%) (Box 3). A complete of 411 individuals have been referred for ICA as elective outpatients (40.4%). Of the 606 individuals transferred between regional and Perth hospitals (inter‐hospital transfers; 59.6%), the indication was NSTEMI in 425 circumstances (70.1%) and chest ache with regular troponin ranges in 132 (21.8%).
Coronary artery illness: traits
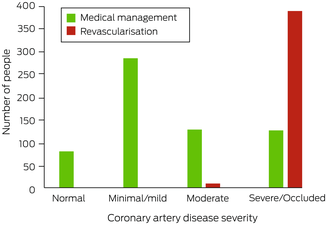
Eighty of the 1017 individuals who underwent ICA had no coronary artery stenosis (7.9%), 285 had minimal or delicate CAD (28.0%), 137 had average CAD (13.5%), and 515 had extreme CAD or an occluded vessel (50.7%) (Box 4). A bigger proportion of individuals with NSTEMI had obstructive CAD (≥ 50% stenosis) than of these with different indications for ICA (327 of 438 [74.7%] v 325 of 579 [56.1%]; OR, 2.3; 95% CI, 1.8–3.0).
Coronary artery illness: administration
After present process ICA, 619 individuals have been medically managed (60.9%) and 398 underwent revascularisation (39.1%; ICA:revascularisation ratio, 2.6). No‐one with non‐obstructive CAD (< 50% stenosis), 9 with average CAD (7%), and 389 with extreme CAD or an occluded vessel (75.5%) underwent revascularisation (Box 5). A bigger proportion of individuals with NSTEMI underwent revascularisation (55%) than of these with chest ache and regular troponin ranges (35%; OR, 2.3; 95% CI, 1.7–3.0) or different indications for ICA (10%; OR, 11; 95% CI, 6.4–18) (Box 6). Twenty‐three individuals skilled peri‐procedural issues (2.3%) (, desk 3).
Health care prices
Total estimated well being care prices for the 1017 individuals who underwent ICA in Perth have been $20.3 million; substantial prices have been related to aeromedical switch (knowledge not proven). The estimated prices by indication have been $12.4 million for NSTEMI (60.9%), $5.4 million for chest ache with regular troponin stage (26.7%), and $2.5 million for different (12.4%) (Box 7). Mean misplaced productiveness for the 612 individuals of working age was 3.4 days (SD, 3.0 days) and the imply revenue misplaced $754.81 (SD, $728.87).
Local computed tomography coronary angiography mannequin of care
Were CTCA undertaken in rural centres, 573 referrals might have been averted (52.7%), the variety of metropolitan hospital mattress‐days diminished from 4065 to 2308 (43% discount), and the ICA:revascularisation ratio diminished from 2.6 to 1.6. Total estimated well being care prices could be diminished from $20.3 million to $13.0 million (36% discount) (Box 8). The value proportion saved was decrease for individuals with NSTEMI as ICA indication ($3.2 million, 26%) than for these with chest ache and regular troponin ranges ($2.4 million, 44%) or different indications ($1.6 million, 64%). Not transferring individuals of working age with non‐extreme stenosis would save a imply 3.0 days (SD, 2.6 days) of misplaced productiveness and $619.90 in misplaced revenue per affected person (SD, $568.00).
Assuming 99% sensitivity and 88% specificity for CTCA detecting obstructive CAD (in contrast with ICA), obstructive CAD could be decided by CTCA in 44 individuals with non‐obstructive CAD (4.3% of individuals assessed with ICA), and obstructive CAD could be missed in seven individuals with obstructive CAD (0.7%) (, desk 4).
Discussion
We report the primary examine of CAD severity in individuals in rural and distant areas of WA referred with non‐pressing indications to metropolitan tertiary hospitals for ICA analysis. More than one‐third of individuals within the examine had regular coronary arteries or non‐obstructive CAD (< 50% stenosis), all of whom have been medically managed. About 75% of individuals with extreme CAD or an occluded vessel underwent revascularisation (389 of 515), however solely 7% (9 of 137) with average CAD (50–69% stenosis); in complete, for each 2.6 ICA assessments undertaken, one affected person underwent revascularisation. We additionally discovered that endeavor CTCA in rural centres might avert 53% of transfers for ICA by regionally figuring out individuals with non‐obstructive CAD who could not require ICA. This would cut back the variety of required metropolitan hospital mattress‐days by 43%, well being care prices by 36%, the ICA:revascularisation ratio from 2.6 to 1.6, and misplaced productiveness by three days per affected person.
As transferring individuals from rural and distant areas to metropolitan hospitals is dear — a big proportion of the full prices are for aeromedical retrieval — pointless transfers needs to be prevented. Not unexpectedly, the prices of inter‐hospital transfers of individuals with NSTEMI accounted for 2‐thirds of all well being care prices. Although a bigger proportion of sufferers with NSTEMI (55%) than of individuals with different indications for ICA underwent revascularisation, nearly half have been medically managed. To enhance useful resource use, scale back the danger of ICA‐associated issues, and minimise inconvenience for sufferers, it’s due to this fact fascinating to regionally determine individuals with non‐obstructive CAD, who could not require revascularisation.
CTCA is a longtime non‐invasive modality beneficial in pointers as a primary line investigation for individuals with secure CAD.14,15 CTCA can also be helpful for assessing individuals with NSTEMI at low to intermediate danger of cardiovascular occasions, given its excessive diagnostic accuracy for ruling out clinically vital CAD, and accuracy equal to that of ICA for assessing long run danger.16,17 Although we included individuals with NSTEMI, CTCA just isn’t thought-about a gatekeeper evaluation for ICA in such circumstances. Local CTCA will not be applicable for all individuals presenting with NSTEMI, notably these at excessive danger of cardiovascular occasions. Indeed, we discovered that the fee financial savings have been decrease when NSTEMI was the indication for ICA, as obstructive CAD and the necessity for revascularisation have been extra seemingly than with different indications. The DISCHARGE trial discovered that the danger of cardiovascular occasions in individuals with secure signs and intermediate chance of obstructive CAD referred for ICA was related whether or not they underwent CTCA or ICA first; nevertheless, a smaller proportion of people that underwent CTCA first skilled main procedural issues (0.5% v 1.9%).18
One benefit of CTCA is that it might detect delicate CAD, enabling clinicians to provoke or intensify preventive therapies. Non‐obstructive CAD is a vital substrate for plaque rupture and myocardial infarction not detected by purposeful testing. The SCOT‐HEART trial discovered that CTCA was related to higher coronary coronary heart illness outcomes for individuals with secure chest ache, most likely due to earlier anatomic characterisation and initiation of medical therapies (eg, aspirin, statins), no matter CAD stage.19
Given the challenges of offering cardiac providers in rural and distant areas,8,20,21 we assist providing CTCA in rural WA to enhance entry to cardiac care and scale back well being care prices. Further, transfers to metropolitan hospitals trigger misplaced productiveness and inconvenience for sufferers. Indigenous individuals, 24% of these referred to metropolitan hospitals for ICA throughout 2019, could also be notably affected by household, cultural, and social disruptions. Investment in CTCA expertise, accreditation, and coaching could be wanted to supply CTCA in rural centres.21
High preliminary prices could possibly be a substantial barrier, and different sensible particulars should even be investigated. On the opposite hand, decreasing the numbers of inter‐hospital transfers and ICA assessments might result in larger effectivity and substantial long run value financial savings. Several components make CTCA extra engaging than different cardiac imaging modalities in rural and distant areas, together with the velocity of picture acquisition, its excessive quantity capability, the comparatively low stage of ionising radiation, and the power to determine non‐obstructive CAD. CTCA may present details about excessive danger plaque, peri‐coronary irritation, cardiac chamber dimension, and diastolic operate.6,7,22
Determining the purposeful significance of average stenosis detected by CTCA might be troublesome. Functional testing is often undertaken to find out the haemodynamic significance of a average stenosis and whether or not ICA is indicated, however such testing is logistically difficult in rural areas, because it requires particular experience and entry to yet one more testing modality. Lesion‐particular ischaemia might be decided by making use of CT‐FFR to the usual CTCA acquisition (with out extra radiation publicity or medicines), and anatomically vital stenoses could possibly be re‐labeled as functionally non‐vital, thereby averting additional purposeful testing and ICA (Box 9).18 CT‐FFR just isn’t used clinically in Australia. however is commercially obtainable within the United States, the United Kingdom, and Japan; within the United States, it’s endorsed for assessing individuals with secure, acute chest ache.15 CT‐FFR might improve the worth of CTCA in rural areas, as its diagnostic efficiency is superior to that of different purposeful exams, it reduces the necessity for ICA, and it predicts affected person outcomes.23,24,25
Limitations
The retrospective nature of our examine and its estimation of prices on the premise of DRG codes have been limitations. The common software of CTCA (as not all contraindications could possibly be recognized) was additionally suboptimal. Although false optimistic CTCA findings might result in probably pointless transfers, the proportion of individuals affected might be small (4.3% of individuals in our examine) and well being care value financial savings would nonetheless be substantial have been they transferred. Moreover, the impression of false positives could be diminished by the addition of purposeful testing in rural areas for individuals with average stenoses, as proposed in our care mannequin.12 Our estimated prices for CTCA in rural areas didn’t embody prices for upgrading scanner software program for 64‐slice CT scanners, sustaining gear, or coaching radiographers and knowledgeable readers, as correct estimates couldn’t be obtained for every rural website. Conversely, financial savings could be increased have been the prices of sufferers ready in rural centres for switch and the impression on metropolitan hospital mattress circulate for avoidable admissions taken under consideration.
Conclusion
About one‐third of individuals in rural and distant WA referred for ICA analysis of CAD throughout 2019 had non‐obstructive CAD, and nearly two‐thirds have been medically managed. By figuring out individuals who could not require ICA, endeavor CTCA in rural centres might avert 53% of referrals to metropolitan hospitals, scale back the variety of metropolitan hospital mattress‐days by 42%, scale back well being care prices by 36% ($7.27 million saved), scale back the proportion of ICA assessments that don’t result in revascularisation, and save three days of misplaced productiveness per affected person. The value‐effectiveness and medical impression of this mannequin of care needs to be prospectively evaluated.
Box 1 – Alternative care mannequin: native computed tomography coronary angiography for individuals in rural or distant areas of Western Australia
Box 2 – People in rural or distant Western Australia assessed for cardiac condtions throughout 2019: choice for inclusion in our examine
Box 3 – Baseline traits of 1017 individuals from rural or distant Western Australia who underwent invasive coronary angiography in Perth throughout 2019*
|
Characteristic |
Number |
||||||||||||||
|
|
|||||||||||||||
|
Total variety of individuals |
1017 |
||||||||||||||
|
Age (years), imply (SD) |
62 (13) |
||||||||||||||
|
Sex (males) |
680 (66.9%) |
||||||||||||||
|
Indigenous individuals |
245 (24.1%) |
||||||||||||||
|
Inter‐hospital transfers |
606 (59.6%) |
||||||||||||||
|
Indication for invasive coronary angiography |
|||||||||||||||
|
NSTEMI |
438 (43.1%) |
||||||||||||||
|
Chest ache with regular troponin stage |
394 (38.7%) |
||||||||||||||
|
Valvular coronary heart illness |
76 (7.5%) |
||||||||||||||
|
Pre‐operative evaluation |
27 (2.6%) |
||||||||||||||
|
Arrhythmia |
23 (2.3%) |
||||||||||||||
|
Cardiomyopathy |
59 (5.8%) |
||||||||||||||
|
|
|||||||||||||||
|
NSTEMI = non‐ST section elevation myocardial infarction; SD = customary deviation. * For referrals by area, see , determine 2. |
|||||||||||||||
Box 4 – Severity of coronary artery illness in 1017 individuals from rural or distant Western Australia who underwent invasive coronary angiography in Perth throughout 2019, by indication
|
Coronary artery illness severity (stenosis) |
|||||||||||||||
|
Indication for invasive coronary angiography |
Number of individuals |
Normal |
Minimal/delicate (< 50%) |
Moderate (50–69%) |
Severe (70–99%) |
Occluded (100%) |
|||||||||
|
|
|||||||||||||||
|
All indications |
1017 |
80 (7.9%) |
285 (28.0%) |
137 (13.5%) |
378 (37.2%) |
137 (13.5%) |
|||||||||
|
NSTEMI |
438 |
27 (6.2%) |
84 (19%) |
35 (8.0%) |
218 (49.8%) |
74 (17%) |
|||||||||
|
Chest ache with regular troponin stage |
394 |
25 (6.3%) |
126 (32.0%) |
69 (18%) |
134 (34.0%) |
40 (10%) |
|||||||||
|
Other* |
185 |
28 (15%) |
75 (40%) |
33 (18%) |
26 (14%) |
23 (12%) |
|||||||||
|
|
|||||||||||||||
|
NSTEMI = non‐ST section elevation myocardial infarction. * Valvular coronary heart illness, pre‐operative evaluation, arrhythmia, cardiomyopathy. |
|||||||||||||||
Box 5 – Management of 1017 individuals from rural or distant Western Australia who underwent invasive coronary angiography in Perth throughout 2019, by severity of coronary artery illness
Box 6 – Management outcomes of 1017 individuals from rural or distant Western Australia who underwent invasive coronary angiography in Perth throughout 2019, by indication for referral
|
Treatment |
|||||||||||||||
|
Indication for invasive coronary angiography |
Medical administration |
Revascularisation |
|||||||||||||
|
|
|||||||||||||||
|
NSTEMI |
197 (45.0%) |
241 (55.0%) |
|||||||||||||
|
Chest ache with regular troponin stage |
256 (65.0%) |
138 (35.0%) |
|||||||||||||
|
Other* |
166 (89.7%) |
19 (10%) |
|||||||||||||
|
|
|||||||||||||||
|
NSTEMI = non‐ST section elevation myocardial infarction. * Valvular coronary heart illness, pre‐operative evaluation, arrhythmia, cardiomyopathy. |
|||||||||||||||
Box 7 – Total well being care prices for 1017 sufferers from rural or distant Western Australia who underwent invasive coronary angiography in Perth throughout 2019, by care mannequin
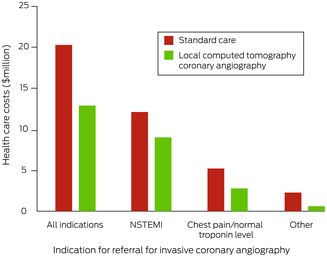
Box 8 – Total well being care prices for 1017 sufferers from rural or distant Western Australia who underwent invasive coronary angiography in Perth throughout 2019, by indication
|
Care mannequin |
|||||||||||||||
|
Indication for invasive coronary angiography |
Standard care |
Alternative mannequin |
Difference |
||||||||||||
|
|
|||||||||||||||
|
All indications |
$20.31 million |
$13.04 million |
–$7.27 million (35.8%) |
||||||||||||
|
NSTEMI |
$12.36 million |
$9.13 million |
–$3.24 million (26.2%) |
||||||||||||
|
Chest ache with regular troponin stage |
$5.42 million |
$3.02 million |
–$2.41 million (44.4%) |
||||||||||||
|
Other* |
$2.52 million |
$0.90 million |
–$1.62 million (64.3%) |
||||||||||||
|
|
|||||||||||||||
|
NSTEMI = non‐ST section elevation myocardial infarction. * Valvular coronary heart illness, pre‐operative evaluation, arrhythmia, cardiomyopathy. |
|||||||||||||||
[adinserter block=”4″]
[ad_2]
Source link